Poster Presentation The Joint Annual Scientific Meetings of the Endocrine Society of Australia and the Society for Reproductive Biology 2017
Improved glycaemic control with carbohydrate counting for adjustment of fast-acting insulin aspart versus insulin aspart in subjects with type 1 diabetes (#226)
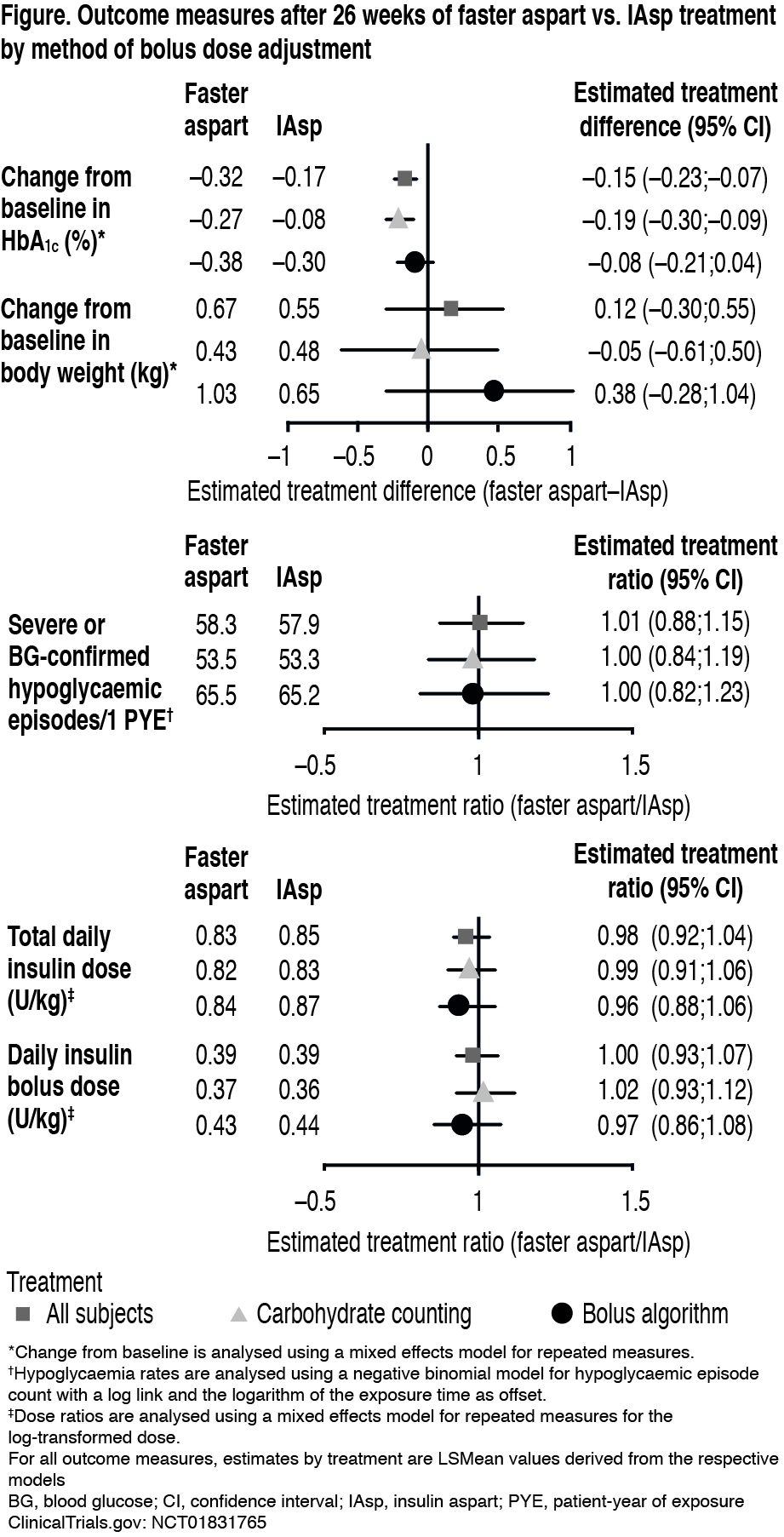
Insulin delivery based on carbohydrate counting (CC) is the gold standard for improving glycaemic control in type 1 diabetes (T1D). A post hoc analysis of onset 1, a 26-week, phase 3 trial, assessed methods for adjusting the dose of mealtime fast-acting insulin aspart (faster aspart) and insulin aspart (IAsp), each with insulin detemir. Subjects with previous experience continued CC (baseline HbA1c, faster aspart and IAsp 7.6%) and the remaining subjects used a simple bolus algorithm (BA; baseline HbA1c, faster aspart 7.5%, IAsp 7.6%).
Faster aspart showed a statistically significant greater reduction in HbA1c vs. IAsp, and non-inferiority was confirmed (Figure). With CC, HbA1c reduction was statistically significantly greater for faster aspart vs. IAsp (estimated treatment difference: −0.19% [95% confidence interval: −0.30;−0.09]) but was similar for both treatments with a BA. The rates of hypoglycaemic episodes and bolus insulin dose were similar between treatments across adjustment methods. No significant differences in total insulin dose or weight gain were observed between treatments with either adjustment method.
Faster aspart was effective in glycaemic control regardless of adjustment method. For patients with T1D capable of dosing based on CC, faster aspart may offer improved glycaemic control vs. IAsp, with similar weight gain and insulin dose, and without an increased risk of hypoglycaemia.
ClinicalTrials.gov: NCT01831765